Health facility patients and residents are very vulnerable to the physical environment. Mental health patients may be even more so. From our own experience we know that a chaotic environment can be more challenging when we are stressed.
Apart from speaking with and observing mental and behavioural clients, we can inform the design process by embracing the tenets of environmental psychology. Environmental psychology is the study of the impact of physical settings on the human experience. If we address the fundamentals of environmental psychology, rather than embrace generic solutions, we will more effectively support patients. For example, researchers often recommended that all inpatient rooms be private, however, the actual goal is to reduce infection, allow the patient to manage social interactions, and control noise. If these latter goals can be kept in mind, communities that cannot afford private rooms can focus on creative, culturally appropriate, alternatives.
The following ten psychologically-related goals have been consolidated and derived from Design for Mental and Behavioural Health, and are discussed in more detail in that publication.
Providing choice and control may be the most critical factors in providing a psychologically supportive environment and most of the other goals discussed here are associated with this concept. Experiences resulting in feelings of lack of control are very common among patients. The importance of providing a sense of control in healthcare settings has been mentioned by Ulrich and noted as a critical factor in providing patient-centred care by Devlin and Arneill. Offering choices increases an individual’s sense of control and thereby reduces stress. Relatedly, feelings of autonomy and spontaneity, might enhance choice and control and could be addressed by patient-manipulated environmental features.
When thinking about choice and control we should also recognise the needs of staff. Healthcare staff are most effective when their own personal needs are addressed. Mental health staff face additional challenges due to the frequency of patient aggression. Therefore, retreat and therapy spaces for staff mental health should be considered in a facility.
Robert Sommer defines personal space as “an area with invisible boundaries surrounding a person’s body into which intruders may not come”. Personal space is the unconscious spatial envelope around an individual that defines relationships with others. Privacy is linked to personal space but focuses on our ability to control social interaction. Potentially, privacy and appropriate social density can be linked to treatment protocols. Additionally, the ability of patients to embellish their environment with personal identifiers may support emotional attachment through personalisation. Design teams should be aware of the role of culture, ethnicity and race on spatial density and personal space needs.
Psychologists describe our interaction with the physical world as ranging in complexity from sensation to perception to cognition. When we think of sensation (taste, sight, smell, hearing or touch), we are referring to our spontaneous response to a sensory stimulation such as awareness of a sound. Perception is considered to be more complex as it might require interpretation of spatial information, such as determining the distance between two objects. Cognition is associated with problem-solving and the conscious manipulation of information. As an example, you might hear a loud noise (sensation), recognise its source as being in the next room (perception) and interpret its meaning as a fallen glass (cognition). The fallen glass might be further processed to provoke fear of violence.
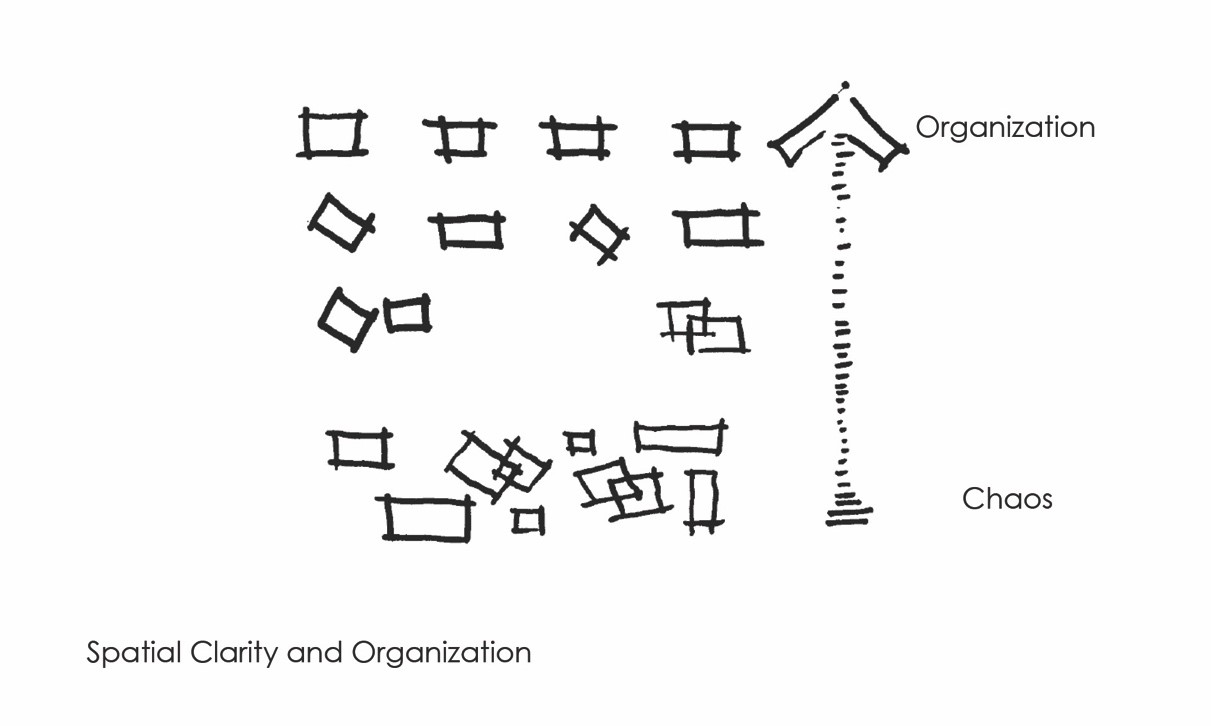
As we stated in Design for Mental and Behavioural Health, “making sense of the world is a primary objective of functioning comfortably in the physical environment.” Spatial clarity and clear organisation are typically reassuring to those facing challenges to their sense of control. Environments that support these factors have been associated with higher patient satisfaction.
Wayfinding is the most recognised expression of spatial clarity. Most designers are aware of the importance of wayfinding, which extends beyond path of travel and incorporates our understanding of territorial markers separating public from private space. The use of signage should only be supplemental to helping people find their way. More importantly, designers should configure buildings in such a way as to provide clues as to how to negotiate a building. These clues might include landmarks such as views outside and artwork or the massing of a building that communicates internal functions. Views outside can also provide reassurance by offering both prospect and refuge – a view of the world from the safety of a protected location within a structure.
While not typically discussed as a tenet of environmental psychology, a deinstitutionalised environment is often preferred by patients. However, a homelike environment embodies the terms previously discussed, i.e., a homelike environment might be perceived as easier to control, provide opportunities for privacy, etc. Sharing bedrooms with strangers would likely be the antithesis of a homelike environment.
Homelike is not a universal aesthetic. Different cultures embrace different representations and for some patients a culturally-inappropriate interpretation of home might seem alien. Additionally, for some patients an environment that resembles their home might be frightening as it could have been the location for negative events. One way to support a comfortable, homelike environment is to provide the backdrop for personalization of space and address Spivak’s 13 activities of daily living: shelter, sleep, mate, groom, feed, excrete, store, territory, play, route, meet, compete and work.

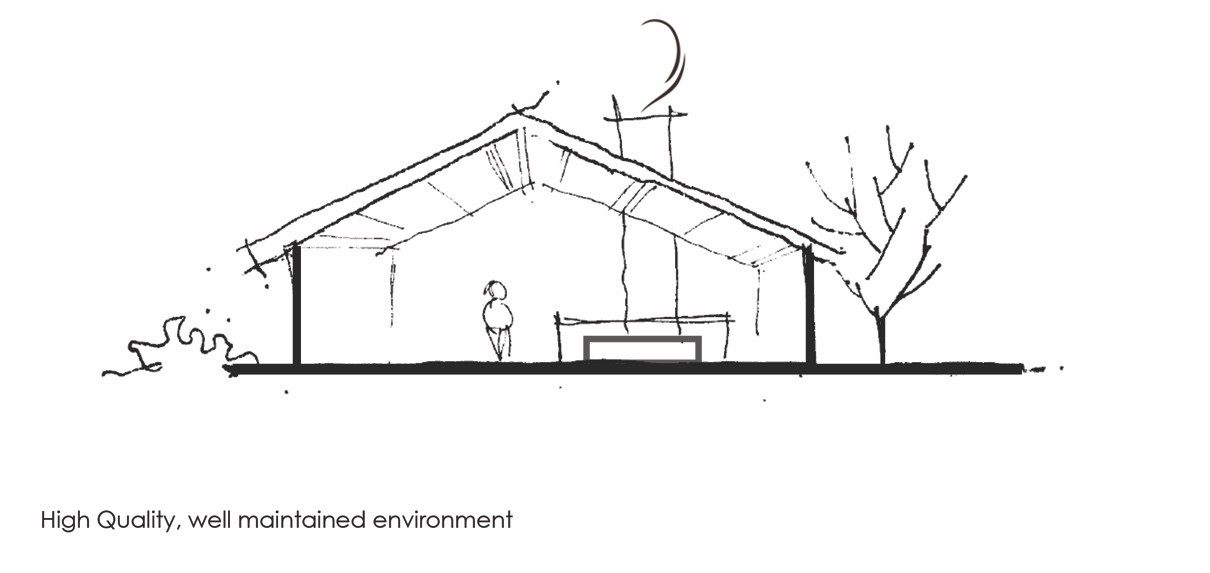
In this case, rather than aesthetics, a high-quality environment refers to an environment constructed of materials that are long-lasting and not easily subject to vandalism. These environments are easier to maintain and, in the long term, less expensive. A high level of maintenance reflects caring on the part of an organisation, an institution’s fiscal stability, and the commitment employees have to their mission.
The challenge is in providing materials that are non-institutional and yet homelike. Researchers have found that patients are more inclined to vandalise institutional-looking finishes and furniture.
As might be expected, several studies have shown that staff and patients express a high preference for well-maintained space. This preference is likely related to the desire for a clear and organised environment, which was discussed previously.
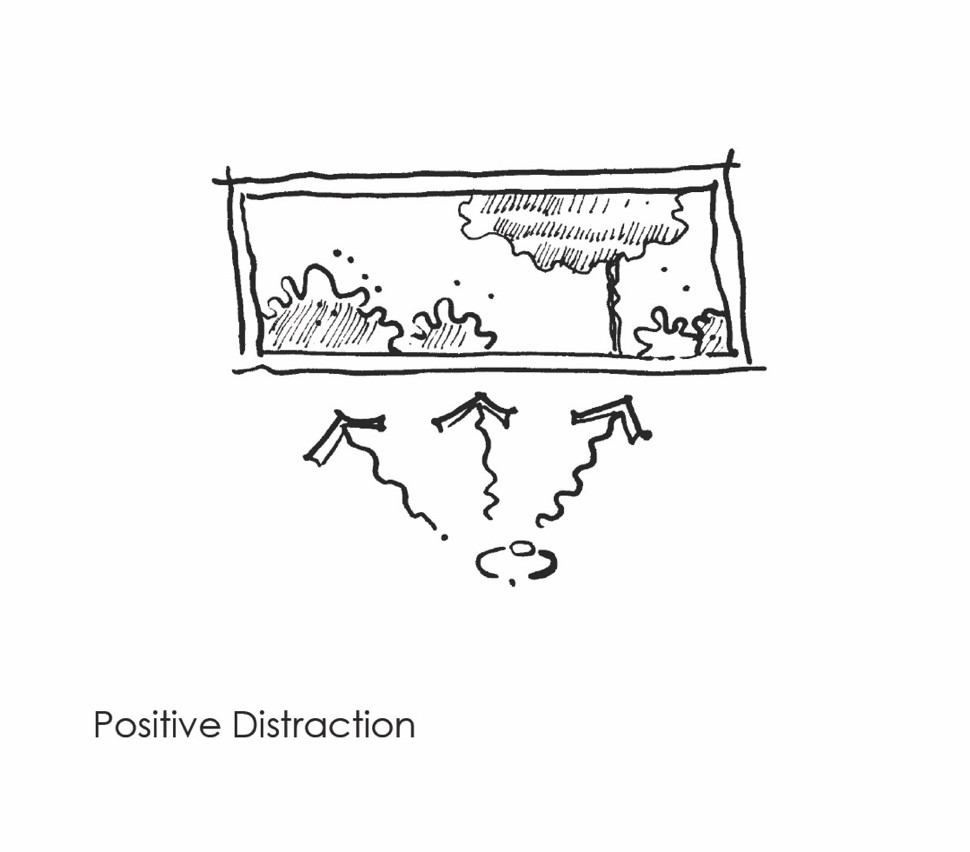
Positive distractions are allow an individual to focus on pleasant experiences rather than the potentially disconcerting experiences associated with healthcare settings. There are a variety of sources of positive distractions, generally falling into three categories, 1) those that involve real-time, real-space dynamic engagement such as social interaction, sports and physical recreation, and interaction with nature; 2) those that involve passive engagement such as music, books, magazines, art and views of nature, and 3) those that involve human-generated, media-focused artifacts, such as TV/streaming, internet use and gaming. The interactions with these distractions can involve physical engagement (such as gaming), but their abstraction from real-time and real-space make the a special area of interest.
The role of art has been controversial as figurative art is thought to be more appropriate than contemporary art. However, contemporary art is widely diverse in its attributes and the best solution is to allow patients to select their own art. Social interaction and access to nature are addressed separately in the following two sections, due to their importance.
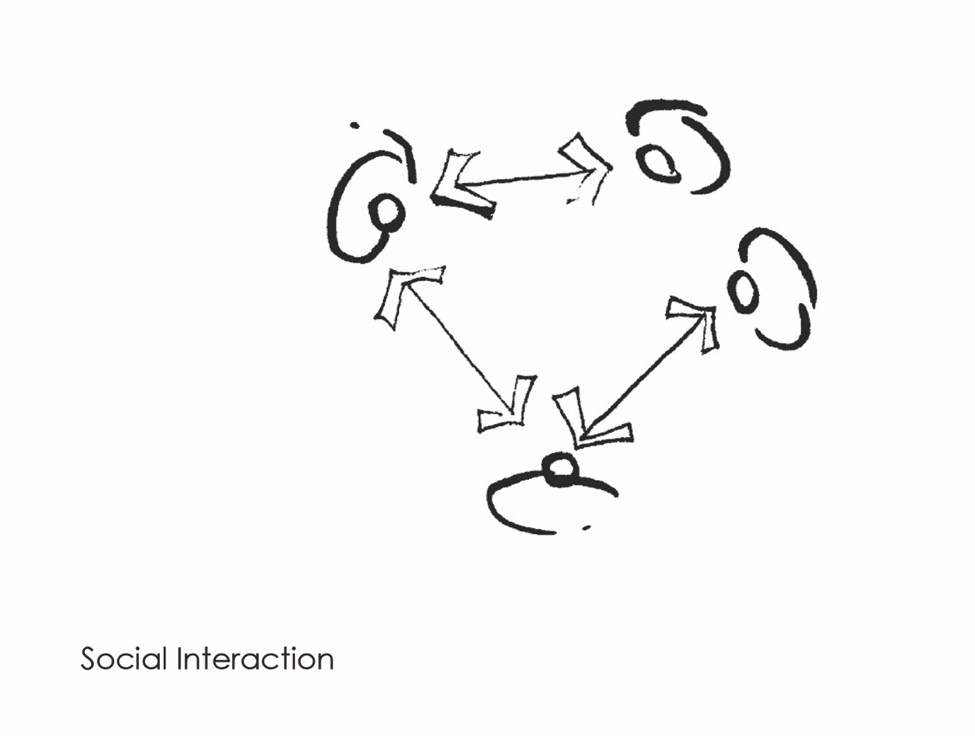
Researchers have found that caring for others, as well as receiving care from others, positively impacts health and longevity. Social interaction and collaboration has been critical from an evolutionary perspective, as these interactions were critical to support the raising of off-spring and for hunting and gathering.
In the context of mental and behavioural health facilities, the provision of spaces for group and dyad interactions will likely be useful for therapeutic programmes. Providing options in shared inpatient areas, through a variety of flexible furniture arrangements, will enable choice and control regarding social interactions. Flexible arrangements in outpatient waiting areas will also facilitate comfort.
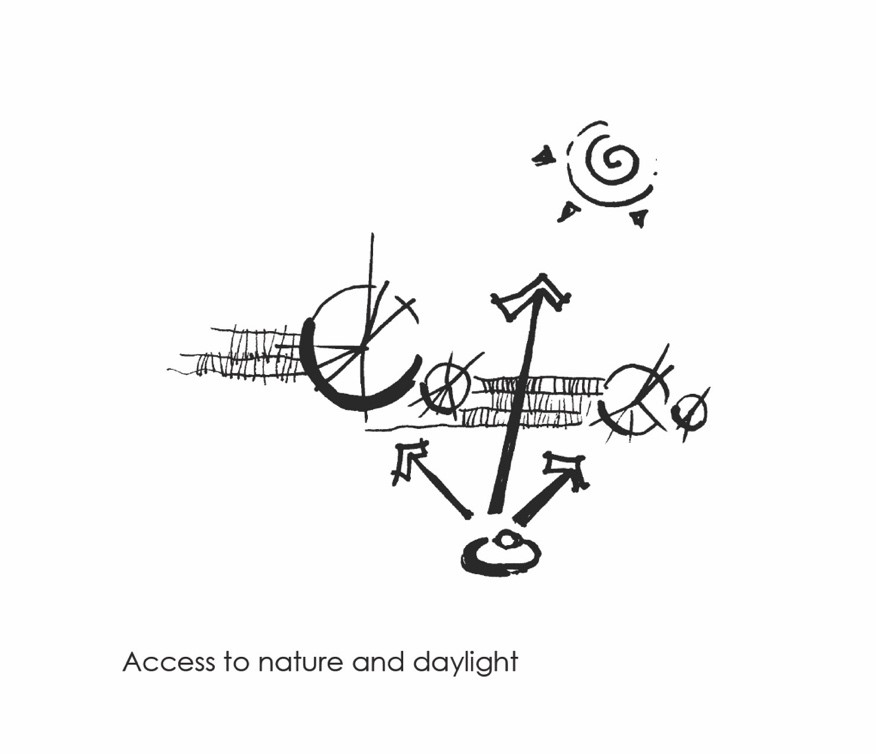
Access to nature, both direct and indirect, has been demonstrated to be very effective in reducing stress. Direct access to nature might manifest itself in terms of parks, gardens or even walks along a tree-lined street. Interactions with animal life is part of this experience. Direct access provides the highest level of engagement, but might require special supervision depending on the acuity of the patients. Horticultural therapy has been an effective tool in a variety of mental and behavioural environments at most acuity levels.
Indirect access, through nature photography or figurative works of art is also enjoyed by mental health patients. This experience can be visual and audial to enhance the experience.
The presence of daylight alone has resulted in beneficial outcomes, likely resulting from both the direct physiological benefits of exposure to sunlight and the psychological benefits from our awareness of diurnal variation. These circadian rhythms likely contribute to our sense of choice and control as they organise our world from a time perspective.
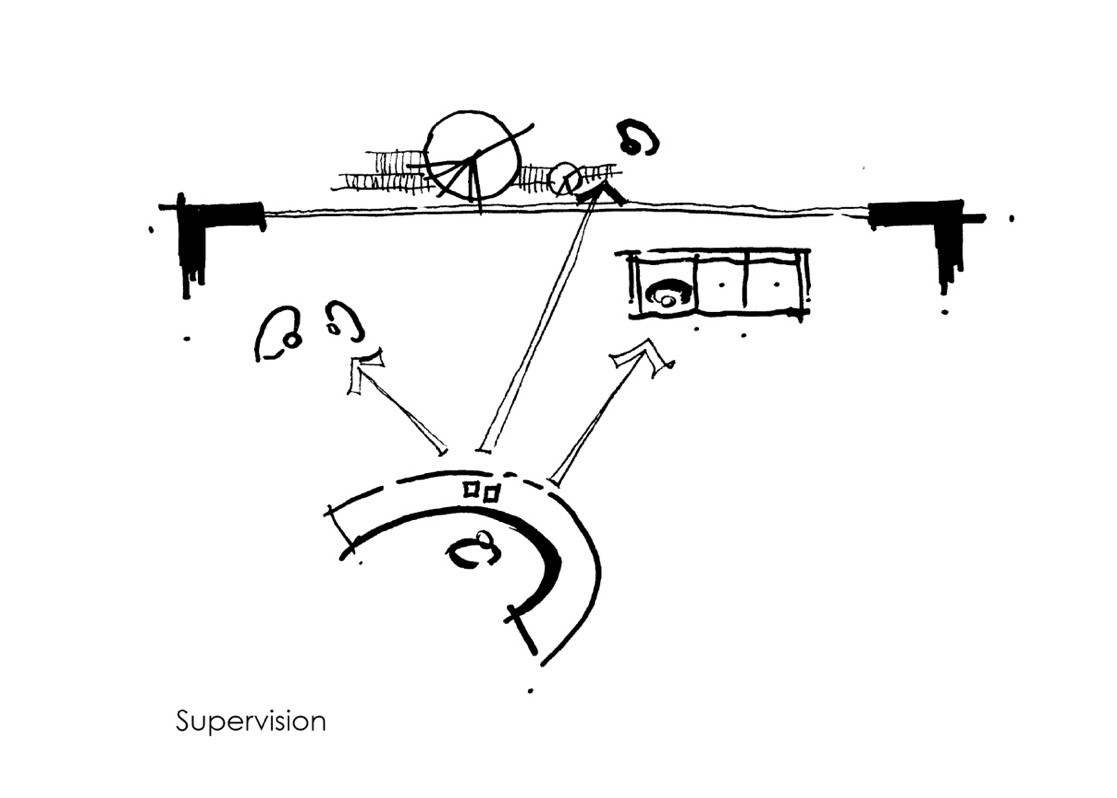
Safety and security are contributors to providing a sense of control. While supporting therapeutic activities, an effort should be made to address patient aggression, absconding and impulsive behaviour. Staff safety and security is impacted by both operational and physical environmental features. Ready supervision is critical to the safety of both patients and staff as aggression is a common event in many psychiatric facilities. There are multiple ways to achieve this. For example, researchers have found that open nurses’ stations are associated with fewer acts of aggression.
Article by Mardelle M Shepley
Narrative & illustrations: Shepley, M. M., & Pasha, S. (2017). Design for mental and behavioral health. Routledge.
